Hello fellow CMIOs, CNIOs, and other Applied Clinical Informatics friends,
This month I'd share some cool discoveries I've made with some friends recently, in a helpful blog post about finding the Clinical Informaticist(s) in your organization, and/or identifying the need for them.

One of the common challenges of Applied Clinical Informatics is that Informaticists can sometimes be hard to find. Typically due to a number Human Resources (HR) and other industry issues, they can sometimes be hidden behind :
- FALSE NEGATIVES - E.g. People who actually do Clinical Informatics work, but aren't necessarily titled "Clinical Informaticist" in their job title, or aren't recognized as doing Clinical Informatics work at all.
- FALSE POSITIVES - E.g. People who are called "Clinical Informaticist", when they don't necessary do the work that might commonly fall under the domain of the Clinical Informaticist (or they only do a specialty branch on the larger 'tree' of Applied Clinical Informatics - See below.)
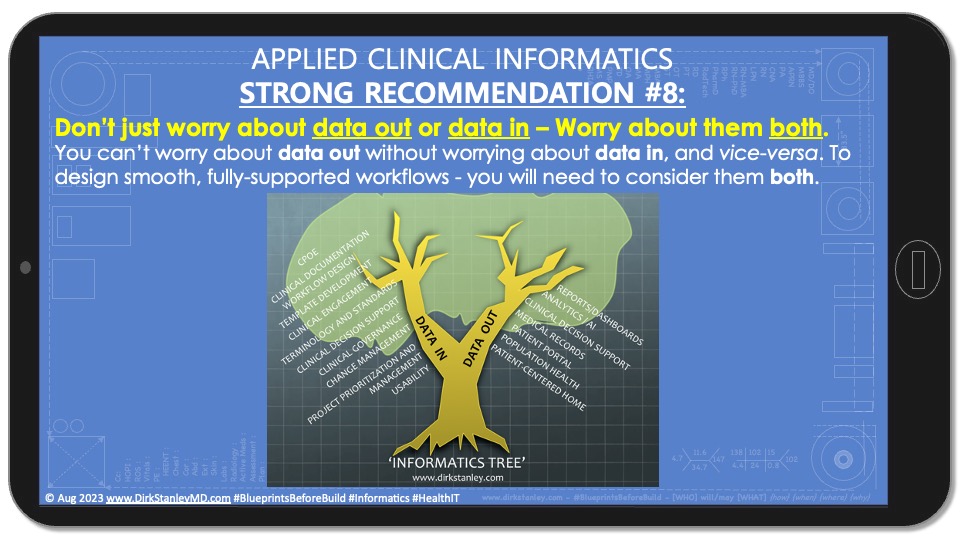
While some have tried to tackle these HR challenges, concrete job descriptions are hard to find since there is such a wide variation of practice, in the general 'tree of Informatics' - which spans a number of disciplines related to both data storage ('data in') and data retrieval ('data out') functions :

If your search for a Clinical Informaticist turns up negative, you will probably need to establish the need to hire one (or more) to help with your clinical workflow analysis and development. Historically, there have been two common approaches to doing this in #Healthcare - the 'Clinical Choir' approach, and the 'Executive/Financial' Approach:

Each of these historic approaches come with some pros and cons :
- The 'Clinical Choir' Approach - Where the Clinical Staff recognizes the need for workflow updates and redesign, and collectively asks for Applied Clinical Informatics resources. PROS : Support from clinical end-users can be very helpful to support the allocation of FTE(s) for Clinical Informatics. CONS : Difficult to execute. Most clinical end-users aren't familiar with the potential role of Applied Clinical Informatics in their day-to-day workflows, so it's not easy to get them to ask for it by name.
- The Executive / Financial Approach - Where the Executive / Finance teams recognize the need for improved Return on Investment (ROI) and overall improved stewardship of technology investments, and so they collectively ask for Applied Clinical Informatics resources. PROS : Support from Executives and Finance officers can also be helpful to support the allocation of FTE(s) for Clinical informatics. CONS : Most ROI from workflow design and improvement falls under the category of 'soft ROI' which could easily be attributed to other departments, or it falls into the category of cost reduction rather than revenue improvements. (Both will help your organization, but one is easier-to-identify.) So putting a hard number to ROI or cost reduction that stands up to scrutiny will require some real pre-planning before you execute your improvement projects.
So for today, I'd like to share a new approach that I recently discovered, when I worked with some of my trusted Project management and Compliance colleagues (Jim McGennis and Elle Box) to combine my 10-step change management recipe with a Responsibility Assignment (RACI) Matrix :

First, a brief reminder that my recommended ten steps for clinical change management (originally published back in 2018) helps to create consistent outcomes through the thoughtful analysis, scoping, development, and planning of workflow changes (both big and small) :

After combining these ten change steps (above) with a Responsibility Assignment (RACI) Matrix (typically used by experienced Project Managers for assigning responsibility for various tasks), new discoveries were made and additional clarity was achieved. (Note : If you're new to Responsibility Assignment / RACI matrices, please see this Wikipedia article for a helpful introduction. And special thanks to PM guru Jim McGennis, for introducing me to this powerful tool.)
The basic premise of a RACI matrix is that you create a grid (spreadsheet) of roles versus steps, and then assign these four categories in each step :
- (R)ESPONSIBLE (also recommender) - The one (or more) person(s) who are responsible to complete the task.
- (A)CCOUNTABLE (also approver or final approving authority) - Who is ultimately answerable for the correct and thorough completion of the deliverable or task, who also ensures the prerequisites of the task are met, and delegates the work to those responsible.
- (C)ONSULTED (sometimes consultant or counsel) - Those whose opinions are sought, typically subject matter experts (SMEs), and with whom there is two-way communication
- (I)NFORMED (sometimes informee) - Those who are kept up-to-date on progress, often only on completion of the task or deliverable, and with whom there is just one-way communication.
Putting my 2018 clinical change management recipe together with the RACI matrix has been remarkably helpful and enlightening. And with some help from Compliance colleages (thanks to Compliance guru Elle Box for her help reviewing and refining the descriptions), the first thing I began to notice was the number of roles that participate in one or more steps of change management :
Roles that participate in one or more steps of clinical change management

Roles that participate in one or more steps of clinical change management
... as well as the details of exactly who is (R)esponsible, (A)ccountable, (C)onsulted, and (I)nformed at each step. (*Note : In the slide above, you'll notice that the Applied Clinical Informaticist already has a different set of roles and responsibilities than the Clinical IT Analysts. More to come on this shortly...)
When we look at the first phase of the change recipe (documentation of request and expectations, or intake) it's easy to see who has primary and secondary (R)esponsibility - Both the clinical end-user and the official requestor - their supervisor, director, chair, or chief - who needs to help support the request :
First phase of change : Documentation of Request and Expectations ('Intake')

First phase of change : Documentation of Request and Expectations ('Intake')
As we move to the second phase of the change management recipe (Analysis, scoping, prioritization, resource allocation, and project approval), we can see that suddenly the Chief Information Officer picks up (A)ccountability, while the Applied Clinical Informaticist has primary (R)esponsibility for the literature search, sponsor identification, workflow gap analysis, workflow development, scoping of deliverables, and identification of stakeholders. Together with a number of (C)onsultants including Clinical IT Analysts, Medical Librarians, Compliance, Regulatory, and Finance, they will also help review regulations and estimate a Total Cost of Ownership (TCO) and Return-on-Investment (ROI), providing much more helpful information for Senior Executives who will need to prioritize and approve this project before it can be assigned. (*Note : By serving this important workflow analysis role, the Applied Clinical Informaticist will also become a subject matter expert (SME) for other experts who will be (R)esponsible for later steps in the change recipe.)
Second phase of change : Analysis, scoping, prioritization, resource allocation, and project approval

Second phase of change : Analysis, scoping, prioritization, resource allocation, and project approval
When we arrive in the third (Project Planning) phase, now the Executive Sponsor has picked up (A)ccountability, while the Project Manager has primary (R)esponsibility for working with the Applied Clinical Informaticist, Clinical IT Analyst, and others to plan the necessary parts of the project, including Gantt charts, RACI Matrices, and/or other formal project plans :
Third phase of change : Project Planning and RACI Matrix / Gantt Chart Development

Third phase of change : Project Planning and RACI Matrix / Gantt Chart Development
Assuming all of the above phases have been completed, this now brings us to the fourth phase of change - The drafting of workflows, for which the Applied Clinical Informaticist has primary (R)esponsibility, typically in conjunction with the Clinical IT Analyst, Compliance, and the End-users.
Fourth phase of change : Drafting of Workflows

Fourth phase of change : Drafting of Workflows
While some organizations may not yet have implemented blueprints in their development process, this step can be very helpful because :
- Blueprints help to create understanding, align clinical stakeholders, let you conduct tabletop workflow discussions and reviews, and obtain preliminary approvals before the Clinical IT Analysts begin their build (in the next step).
- Once approved, and with a few small changes, blueprints can also become your downtime forms, in case your electronic system is ever down for planned maintenance or other unplanned reasons.
This now brings us to the fifth and sixth phases of change, the building of deliverables and testing of workflows, where the Clinical IT Analyst now has primary (R)esponsibility to build and test the deliverables, typically in conjunction with the Applied Clinical Informaticist and the End User (for end-user acceptance testing).
Fifth and sixth phases of change : Building of deliverables and testing of workflows

Fifth and sixth phases of change : Building of deliverables and testing of workflows
For the seventh phase of change (Final workflow approval), the Applied Clinical Informaticist now assumes primary (R)esponsibility and works to secure the necessary final approvals in conjunction with Senior Leadership and a number of other stakeholders. (*Note that the Executive Sponsor still has (A)ccountability for this step.)
Seventh phase of change : Final Workflow Approvals

Seventh phase of change : Final Workflow Approvals
Finally, for the eighth phase (Communication and Education/Training), ninth phase (Implementation/Publication), and tenth phase (monitoring and support) of change, the Clinical IT trainers, Clinical Education / Training team, Communications Team, and End-Users now all share (R)esponsibility, and typically do their steps in conjunction with the Applied Clinical Informaticist and the Clinical IT Analysts.
Eighth, ninth, and tenth phases of change : Communication, Education, Implementation, Monitoring, and Support

Eighth, ninth, and tenth phases of change : Communication, Education, Implementation, Monitoring, and Support
IN CONCLUSION :
What does this exercise (combining change management recipe with a RACI responsibility assignment matrix) teach us? Five helpful take-home points :
- Clinical change management is a team sport that requires the participation of a large number of stakeholders to work together in a clear, highly-detailed, highly-coordinated fashion, where different roles will be (A)ccountable for some steps, have primary (R)esponsibility in some steps, serve as a (C)onsultant in other steps, and need to be (I)nformed of other steps.
- The roles of the Applied Clinical Informaticist and Clinical IT Analyst are separate and distinct roles that often work together, but serve in distinct and unique capacities, and thus should have separate and distinct job titles and descriptions.
- Before projects are approved, the Applied Clinical Informaticist has primary (R)esponsibility for the analysis, scoping, prioritization, and resource allocation, typically in conjunction with (C)onsulting expertise from the Clinical IT Analyst, End-users, Compliance, Regulatory, Finance, Executive Sponsor(s), and Senior Leadership.
- The Applied Clinical Informaticist also has primary (R)esponsibility for the drafting of workflows (blueprints of deliverables), typically in conjunction with (C)onsulting expertise from the Clinical IT Analysts, Compliance, and End-Users. These blueprints will help to create understanding and alignment, and later serve as downtime forms in the event of a planned or unplanned downtime.
- The Clinical IT Analyst often provides (C)onsulting expertise during earlier analysis and scoping phases of the change, but then assumes primary (R)esponsibility for the building and testing of electronic deliverables, before providing additional (C)onsulting expertise during the implementation phase of the change.
I know there's a lot to unpack here, but I hope this review helps to demystify the process, and helps you look at your own change recipe and the roles that are (A)ccountable for, (R)esponsible for, (C)onsulting on, and (I)nformed of each step. I also hope it helps to dispel the misunderstandings and confusion about the roles of the Applied Clinical Informaticist and the Clinical IT Analyst, two important roles that often work together but each of which require their own skill sets, job titles, job descriptions, and support.
Remember, the above is all a [ DRAFT ] and this blog is for educational and discussion purposes only - Your mileage may vary! Have any feedback or experiences you would like to share? Please feel free to leave comments in the comment section below!