Hi fellow CMIOs, CNIOs, and other Informatics friends,
Today I thought I'd share some materials I delivered in a talk back in 2023 for Dr. Judi Binderman, a really seasoned Clinical Informaticist and good friend of mine. I recently discovered these when going through some old slides. At the time, Dr. Binderman had asked me to speak briefly to her team at Community Medical Centers in Fresno, CA about some helpful tips and tricks of clinical workflow redesign :


The first point that I usually emphasize for any new Clinical Informatics leaders is that work can be measured and estimated through a workflow gap analysis. The distance from the current state to the future state gives you a good estimate of the stakeholder(s) you will need to involve in a project, what they will need to learn and do (to achieve your future state), and so this gives you a good estimate of your project deliverables and project scope (for planning purposes) :

Once you have completed your gap analysis to get a sense of the current-state and future-state workflows, you can then review a list of common deliverables, to select what you will need to get your users from current to future state :

Note that some of these deliverables (above) are inside of the Electronic Health Record (EHR), and other deliverables are outside of the EHR. You will want to identify all of the deliverables you anticipate needing/using, and then identify who you will need on your project team to help develop each deliverable.
Remember that workflow change management is a team sport - A common mistake is to think that you can make a change with 'only Doctors' or 'only Nurses'. Almost all clinical workflows depend on many stakeholders, from different enterprises, with a number of different roles. Understanding the different enterprises of your organization, and the different roles you may engage with, is helpful to make sure you've thought through all of the stakeholders you will need to make your project successful :

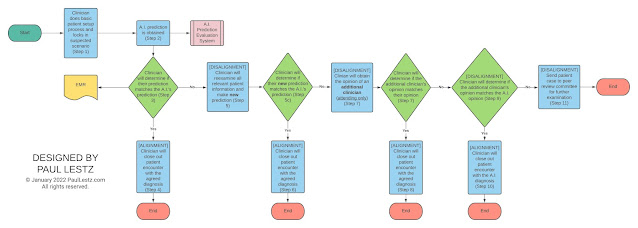
Once you have a sense of the estimated stakeholders and deliverables, it's helpful to think through the steps you will need to develop your workflow. For teaching purposes, I usually shrink this down into ten (10) easy steps, that you can talk through with your development team :

- Waterfall Methodology - Linear, step-by-step, good for plan-first approach, takes longer but especially well-suited for Healthcare or new high-risk scenarios where one build is all you can plan for.
- Agile (Software Development) Methodology - Iterative, emphasizes rapid feedback and adaptation, sometimes useful when clinical workflows are evolving or need user-centered design - but not ideal for Healthcare scenarios. Better built for speed and iterations.
Some people will argue that Waterfall can take too long, and they prefer the speed and flexibility of Agile. Personally, I'm not sure how well Agile fits into the many high-risk clinical workflows of Healthcare (since there is usually little room for error), and so I've condensed those ten (10) helpful steps in the slide above into this 'general-purpose change recipe' below :


This Responsibilty Assigment (RACI) Matrix can then walk you through the first step of your change management - Documentation of Request and Expectations ('Intake') - And help you to develop key questions that your requestor and their supervisor (e.g. Chief, Chair, or Director) can answer before you do further analysis.
Once you have their preliminary input and feedback, you (Clinical Informaticist) can then pursue the next steps of your journey - Analysis, scoping, prioritization, resource allocation, and project approvals - To help evaluate and develop the request, and make sure your Clinical and Administrative Leadership have the information they need to prioritize and approve the project :

- the project priority, estimated scope, estimated stakeholders, estimated deliverables, and necessary resources,
- the estimated Total Cost of Ownership (TCO) and Return on Investment (ROI)


Q : Who is doing what, and in what sequence (order)?
So with a small adaptation, we can revisit the traditional swimlane diagram as :

Procedure (n.) (synonym : workflow, recipe, process, algorithm) - An ordered series of tasks that uses people, time, and resources to achieve a desired goal or outcome.
Now, if you accept the definition above as true, then you can create a simple template for writing a task, the most basic building block of a procedure (synonym : workflow, recipe, process, algorithm) :
Task = [ WHO ] will/may [ WHAT ] { how } { when } { where } { why }
where :
- [ WHO ] = Role of the person that will perform the task
- will/may = Use "WILL" for required tasks, "MAY" for optional tasks
- [ WHAT ] = Brief description of the task
- { how } = Optional modifier, use only when needed to clarify how the task is performed
- { when } = Optional modifier, use only when needed to clarify when the task is performed (for timing/duration)
- { where } = Optional modifier, use only when needed to clarify where the task is performed
- { why } = Optional modifier, use only when needed to clarify why the task is formed
You can then include this in your own 'workflow glossary', where you define and organize your favorite high-grade (policy-grade) terminology related to workflow design :




- Cost = Labor + Materials
- Cost = (Salary * Time) + Materials
... to each step :








I hope this has been a helpful journey into how to document, analyze, and develop your own clinical workflows. If you have any questions, please feel free to leave them in the feedback/comment section below! (And special thank you to both Dr. Judi Binderman and Dr. Charles Webster for their contributions to this post!)
REMEMBER : This blog is for education and discussion purposes only - Your mileage may vary. Have any other helpful tricks for quickly untangling or developing clinical workflows? Feel free to leave them in the comments section below!